International Journal of Periodontics & Restorative Dentistry, Pre-Print
DOI: 10.11607/prd.7179, PubMed-ID: 3905894426. Juli 2024,Seiten: 1-15, Sprache: EnglischUrban, Istvan A. / Di Martino, Maria / Rangel, Rodrigo / Latimer, Jessica / Forster, Andras / Tavelli, LorenzoA 45-year-old female patient presented with a lack of inter-implant papilla after a partially edentulous anterior area was rehabilitated with dental implants. The soft tissue phenotype and inter-implant papilla was augmented using the “iceberg” connective tissue graft, followed by a second surgical procedure where a strip gingival graft was combined with a connective tissue graft inserted underneath a pouch prepared into the previous “iceberg” connective tissue graft at the level of the crest (“garage” approach), further enhancing soft tissue volume in that region. This technique aims to improve mucosal thickness and supracrestal tissue height while addressing esthetic concerns associated with multiple implant placements in the anterior region. The final esthetic outcome was excellent, harmonious soft tissue with appropriate thickness, symmetry with adjacent teeth, well-shaped interdental and inter-implant papilla with high patient satisfaction, making this approach a valuable addition to a surgeon’s armamentarium. Future clinical studies are needed to evaluate the performance of this novel approach.
International Journal of Periodontics & Restorative Dentistry, Pre-Print
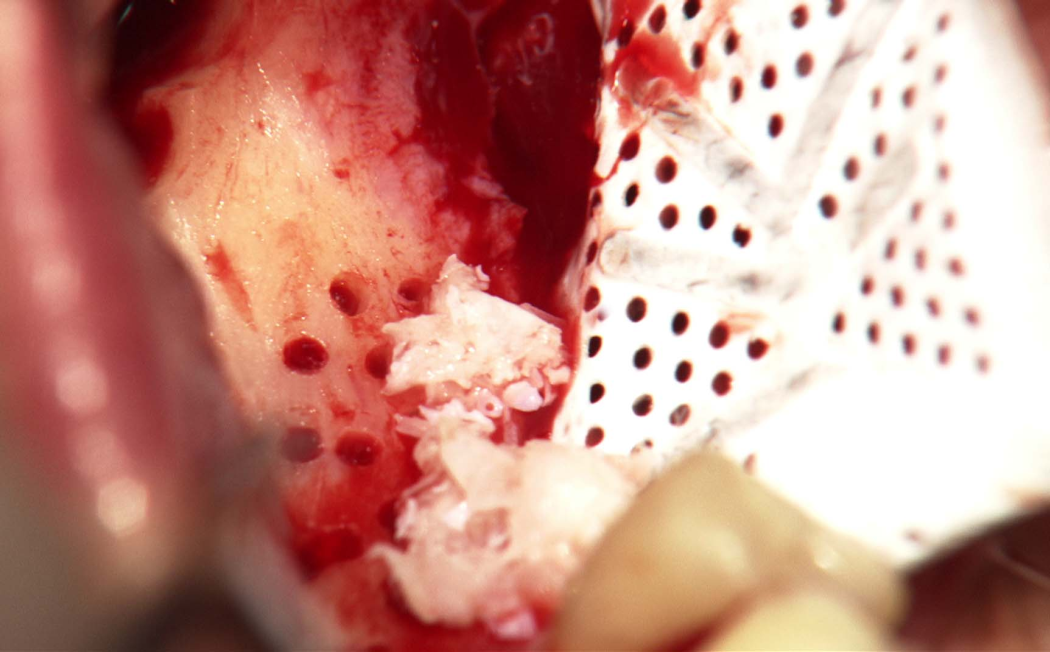
DOI: 10.11607/prd.7110, PubMed-ID: 387272473. Mai 2024,Seiten: 1-27, Sprache: EnglischUrban, Istvan A. / Mirsky, Nicholas / Serroni, Matteo / Tovar, Nick / Vivekanand Nayak, Vasudev / Witek, Lukasz / Marin, Charles / Saleh, Muhammad H. A. / Ravida, Andrea / Baczko, Istvan / Parkanyi, Laszlo / Nagy, Katalin / Coelho, Paulo G.Background: Non-perforated Polytetrafluoroethylene (PTFE) membranes are effectively utilized in guided bone regeneration (GBR) but may hinder cell migration due to limited interaction with the periosteum. This study compared bone regeneration using occlusive or perforated membranes combined with acellular collagen sponge (ACS) and recombinant human bone morphogenic protein-2 (rhBMP-2) in a canine mandibular model. Material and Methods: Male beagle dogs (n=3) received two mandibular defects each to compare ACS/rhBMP-2 with experimental (perforated group) and control (non-perforated group) membranes (n=3 defects/group). Tissue healing was assessed histomorphologically, histomorphometrically and through volumetric reconstruction using microcomputed tomography. Results: The perforated group showed increased bone formation and reduced soft tissue formation compared to the non-perforated group. For the primary outcome, histomorphometric analysis revealed significantly greater total regenerated bone in the perforated group (67.08 ± 6.86%) relative to the nonperforated group (25.18 ± 22.44%) (p = 0.036). Perforated membranes had less soft tissue infiltration (32.91 ± 6.86%) compared to non-perforated membranes (74.82 ± 22.44%) (p = 0.036). Conclusion: The increased permeability of membranes in the perforated group potentially enabled periosteal precursor cells greater accessibility to rhBMP-2. The availability may have accelerated their differentiation into mature bone-forming cells, contributing to the stimulation of new bone production, relative to the non-perforated group.
Schlagwörter: Osteogenesis, periosteum, bone regeneration, polytetrafluoroethylene, implants
International Journal of Periodontics & Restorative Dentistry, Pre-Print
DOI: 10.11607/prd.7476, PubMed-ID: 397757147. Jan. 2025,Seiten: 1-20, Sprache: EnglischUrban, Istvan A. / Mancini, Leonardo / Akhondi, Samuel / Tavelli, LorenzoIt is well known that keratinized mucosa (KM) plays a crucial role for maintaining peri implant health and esthetic outcomes. The Strip Gingival Graft (SGG) technique, which involved an apically positioned flap (APF), in combination with an autogenous SGG and a xenogeneic collagen matrix (XCM), demonstrated its efficacy in re-establishing an adequate amount of KM width at implant sites. Nevertheless, it is still unclear whether harvesting the SGG from the palate (pSGG) or from the buccal aspect of natural dentition (bSGG) affects the esthetic outcomes at the augmented implant sites. Therefore, the objective of the present study was to compare the esthetic outcomes of dental implants augmented with either bSGG + XCM or pSGG + XCM. The present study was designed as a single-center retrospective study, assessing the esthetic and colorimetric outcomes of peri-implant KM augmentation with either pSGG + XCM or bSGG + XCM in cohort of 49 subjects. The two groups were compared in terms of colorimetric outcomes, assessed on clinical photograph using specific software able to identify and quantify the predominant color within the peri implant soft tissue. Colorimetric comparisons with adjacent untreated sites were also investigated. In addition, the Pink Esthetic Score (PES) and the Subjective Esthetic Score (SEE) were performed to further assess the esthetic outcomes of pSGG + XCM and bSGG + XCM. The colorimetric analysis did not show statistically significant differences among sites augmented with pSGG + XCM, sites augmented with bSGG + XCM, and untreated sites. Implants treated with bSGG + XCM showed significantly greater PES (in terms of shape of the mesial and distal papilla, level of the soft tissue margin, soft tissue contour, anatomy of the alveolar process, and final PES) and SEE compared to implants augmented with pSGG + XCM. The present study demonstrated that implant sites augmented with APF with either pSGG + XCM or bSGG + XCM did not show different colorimetric outcomes compared to adjacent untreated sites, while bSGG + XCM obtained superior professional and subjective esthetic scores compared to pSGG + XCM.
International Journal of Periodontics & Restorative Dentistry, Pre-Print
DOI: 10.11607/prd.7205, PubMed-ID: 3882027731. Mai 2024,Seiten: 1-22, Sprache: EnglischUrban, Istvan A. / Chen, Zhaozhao / Wang, Hom-LayPeri-implantitis, a common complication among patients receiving implant-supported restorative
therapy, often requires surgical intervention for effective treatment. Understanding the specific
configuration of peri-implant bony defect and adjacent bone peaks is crucial for tailoring treatment
strategies and improving outcomes. A decision tree for reconstructive peri-implantitis therapy has been
developed based on the new classification of defect configurations (Class I to V), guiding clinicians in
selecting treatment options, including biomaterials, techniques, and healing approaches. Furthermore,
clinicians are encouraged to consider various factors such as local predisposing factors (such as soft
tissue characteristics, prosthetic design, and implant position in three-dimensional perspective), clinical
factors (surgeon skill and experience), and patient-related factors (such as local and systemic health,
preferences, and cost) when evaluating reconstructive therapy options.
Schlagwörter: bone regeneration, dental implants, peri-implant defect, peri-implantitis, reconstructive therapy
International Journal of Periodontics & Restorative Dentistry, 5/2024
DOI: 10.11607/prd.6731, PubMed-ID: 37552185Seiten: 510-519, Sprache: EnglischUrban, Istvan A / Mancini, Leonardo / Wang, Hom-Lay / Tavelli, LorenzoImplants with deficient papillae and black triangles are common findings. The treatment of these esthetic complications is considered to be challenging with limited predictability. Therefore, the present report aims to describe a novel technique for papilla augmentation: the “iceberg” connective tissue graft (iCTG) after extraction and interproximal bone reconstruction in the anterior region. A 35-year-old patient presented with a hopeless tooth with interproximal clinical attachment loss extending to the apical third of the adjacent tooth. Interproximal bone reconstruction was performed through alveolar ridge preservation by directly applying recombinant human platelet-derived growth factor-BB (rhPDGF-BB) to the exposed root surface of the adjacent tooth. A mixture of autogenous bone chips (obtained from the ramus) and bovine bone xenograft particles (previously mixed with the growth factor) was also used. The patient was able to return for implant therapy only 2 years later, at which time an incomplete regeneration of the interproximal bone was observed. Therefore, to compensate the interproximal deficiency, the iCTG approach was utilized, involving a double layer of CTG with different origins. Two small grafts from the tuberosity were sutured to the mesial and distal ends of a wider CTG harvested from the palate, aiming to gain additional volume at the interproximal sites. The composite graft was then sutured on top of the implant platform, and the flap was then released and closed by primary intention. After conditioning the peri-implant tissues, the case was finalized with a satisfactory outcome. The described iCTG could be an effective approach for reconstructing peri-implant papillae following interproximal bone reconstruction.
International Journal of Oral Implantology, 4/2024
PubMed-ID: 39559941Seiten: 411-420, Sprache: EnglischUrban, Istvan / Chen, Zhaozhao / Wang, Hom-LayCase presentation: Although most peri-implant lesions feature a combined defect configuration that involves both supra- and infraosseous components, regenerating the supraosseous part is considered the optimal approach, albeit a challenging one, and often requires vertical bone augmentation. This report provides a detailed description of submerged membrane techniques for vertical bone augmentation around supraosseous peri-implant defects. Cases involving different types of membrane (both resorbable and non-resorbable) with or without the use of bone graft are presented. In the first case, the patient had a mild supraosseous defect that was managed using the sausage technique with collagen matrix soaked with human recombinant bone morphogenetic protein-2. In cases two to five, titanium-reinforced dense polytetrafluoroethylene membranes were employed. Conclusion: The reconstruction of supraosseous peri-implant defects is technique sensitive but can be achieved when adhering to the principles of space maintenance and submerged healing.
Schlagwörter: bone regeneration, dental implants, human recombinant bone morphogenetic protein-2, peri-implantitis, supraosseous defects
The authors declare there are no conflicts of interest relating to this study.
International Journal of Oral Implantology, 3/2024
PubMed-ID: 39283217Seiten: 237-248, Sprache: EnglischZahedi, Ehsan / Saleh, Muhammad H A / Adel-Khattab, Doaa / Gallo, Pier / Levine, Robert / Wang, Hom-Lay / Urban, IstvanDental implants are a reliable treatment option for restoring missing teeth, but adequate bone quantity and quality are crucial for success. This case series presents four cases treated by different clinicians, all following very similar concepts for combined periodontal and vertical ridge augmentation using recombinant human platelet-derived growth factor-BB. All cases involved a severe periodontal defect requiring either extraction of the adjacent tooth or periodontal regeneration. Different bone grafts and membrane types were utilised. Although true periodontal regeneration cannot be said categorically to have occurred due to a lack of histological evidence, the clinical and radiographic findings suggest almost complete bone fill in all cases. This case series demonstrates that combined periodontal and vertical ridge augmentation using recombinant human platelet-derived growth factor-BB could be successful, but proper case selection and patient preparation for the possibility of multiple surgical procedures are recommended.
Schlagwörter: case report/series, complications, growth factors, guided bone regeneration, surgical
At the time of preparing this manuscript, Dr Saleh was a clinical advisor for Lynch Biologics, Franklin, TN, USA.The other authors declare that they have no conflicts of interest relating to this study.
International Journal of Periodontics & Restorative Dentistry, 2/2024
DOI: 10.11607/prd.6458, PubMed-ID: 37722007Seiten: 213-218, Sprache: EnglischShahbazi, Arvin / Windisch, Péter / Tubbs, R. Shane / Decater, Tess / Urbán, István A. / Baksa, Gábor / Iwanaga, JoeGuided bone regeneration (GBR) requires a tension-free flap without damaging the collateral circulation in order to secure better surgical outcomes. Topographic knowledge regarding the neurovascular bundles in the posterior aspect of the mandible can prevent complications during lingual flap design. The lingual branch (LB) of the inferior alveolar or maxillary arteries is not sufficiently illustrated or described in the literature. Nevertheless, it has an intimate relationship with the lingual nerve (LN) during ridge augmentation and implant-related posterior mandible surgery. Therefore, this study aimed to clarify the morphology and topography of the LB related to GBR surgeries. In the present human cadaveric study, the LB was analyzed in 12 hemimandibles using latex injection and corrosion casting. Two types of LB were identified based on their origin and course. The LB was found in a common connective tissue sheath close to the LN. The LB assembled several anastomoses on the posterior lingual aspect of the mandible and retromolar area. The LB acted as an anatomical landmark in identifying LN at the posterior lingual aspect of the mandible.
International Journal of Periodontics & Restorative Dentistry, 1/2024
DOI: 10.11607/prd.6667, PubMed-ID: 37552184Seiten: 17-25, Sprache: EnglischUrban, Istvan A. / Saleh, Muhammad H. A. / Serroni, Matteo / Shahbazi, Arvin / Baksa, Gabor / Szoke, Peter / Ravida, AndreaVertical ridge augmentation in the anterior mandible is a technically delicate procedure that requires knowledge of some anatomical structures to reduce intra- and postoperative complications. Proper soft tissue management is one of the primary aspects to the success of these techniques, enabling tension-free primary wound closure and preventing membrane exposure. This cadaveric and clinical study provides an anatomical overview of the lingual portion of the anterior mandible. Moreover, there is a description of a novel surgical approach for release of the lingual flap that will help clinicians achieve primary closure without incurring intrasurgical complications.
International Journal of Esthetic Dentistry (DE), 4/2023
The Last PageSeiten: 442, Sprache: DeutschUrban, Istvan