Auf unserer Website kommen verschiedene Cookies zum Einsatz: Technisch notwendige Cookies verwenden wir zu dem Zweck, Funktionen wie das Login oder einen Warenkorb zu ermöglichen. Optionale Cookies verwenden wir zu Marketing- und Optimierungszwecken, insbesondere um für Sie relevante und interessante Anzeigen bei den Plattformen von Meta (Facebook, Instagram) zu schalten. Optionale Cookies können Sie ablehnen. Mehr Informationen zur Datenerhebung und -verarbeitung finden Sie in unserer Datenschutzerklärung.
Genauigkeit von Gesamt- und Teilkieferabformungen aktueller intraoraler Scansysteme in vitro
Scannen wird schneller und besser – Systeme liefern bereits Genauigkeiten innerhalb der klinischer Anforderungen
PD Dr. med. dent. Andreas Ender
Ziel: Intraoralscanner (IOS) werden inzwischen häufig für die Herstellung digitaler Modelle direkt am Patienten genutzt. Verbesserungen der IOS werden zusätzlich von Generation zu Generation erreicht. Das Ziel der vorliegenden Studie war eine Beurteilung der Genauigkeit von neuen und aktuellen intraoralen Scansystemen für Gesamt- und Teilkieferabformungen in vitro.
Material und Methode: Ein spezielles Gesamtkiefermodell des Oberkiefers mit Zähnen aus Feldspatkeramik wurde als Referenzmodell verwendet und mit einem Laborscanner (ATOS III Triple Scan MV60) digitalisiert. Die Abformung des Gesamtkiefers erfolgte konventionell mit einem Polyvinylsiloxanmaterial (CO; President) und digital mit acht verschiedenen IOS-Systemen (TRn: Trios 3; TRi: Trios 3 insane; CS: Carestream Dental CS 3600; MD: Medit i500; iT: iTero Element 2; OC4: Cerec Omnicam 4.6.1; OC5: Cerec Omnicam 5.0.0; PS: Primescan) (n = 10 pro Gruppe). Die konventionellen Abformungen wurden mit Typ IV Gips (Fujirock EP) ausgegossen und die Modelle mit einem Laborscanner (inEOS X5) digitalisiert. Alle Datensätze wurden im STL-Dateiformat exportiert und für die weitergehende Analyse in verschiedene Bereiche beschnitten: Gesamtkiefer, vorderes Teilkiefersegment und hinteres Teilkiefersegment. Die Richtigkeits- und Präzisionswerte für die entsprechenden Bereiche wurden in einer 3D-Überlagerungsmethode mit spezieller 3D-Differenzanalyse-Software (GOM Inspect) unter Verwendung von (90-10)/2 Perzentil-Werten evaluiert. Die statistische Auswertung erfolgte mit der One-Way-ANOVA oder dem Kruskal-Wallis Test (α = 0,05). Die Angabe aller Ergebnisse erfolgt als Median-[IQR]-Wert in µm.
Die Zeitschrift soll es dem Praktiker wie dem Wissenschaftler ermöglichen, sich umfassend mit allen Gebieten der computergestützten Zahnheilkunde auseinanderzusetzen, um so das neue Medium Computer nutzbringend in die Behandlungskonzepte integrieren zu können. Das Besondere dieser Zeitschrift ist ihre Mehrsprachigkeit: Alle Artikel werden sowohl auf Englisch als auch in der Muttersprache der Autoren veröffentlicht; die Beiträge englischer Autoren zusätzlich auf Deutsch. Damit wird - unter Wahrung der Originalität - ein international zugängliches Forum des Informationstransfers auf diesem Sektor geschaffen. Mehr Infos zur Zeitschrift, zum Abo und zum Bestellen eines kostenlosen Probehefts finden Sie im Quintessenz-Shop.
Ergebnisse: Die Werte für Gesamt- und Teilkieferabformungen in vitro zeigten statistisch signifikante Abweichungen zwischen den Testgruppen (p < 0,05). Für den Gesamtkiefer lagen die Richtigkeitswerte im Bereich von 16,3 [2,8] µm (CO) und 89,8 [26,1] µm (OC4) und die Präzisionswerte im Bereich von 10,6 [3,8] µm (CO) und 58,6 [38,4] (iT). Im Falle der Teilkieferabformungen wurden für alle Gruppen für das hintere Teilkiefersegment die besten Richtigkeitswerte ermittelt, mit 9,7 [1,2] µm für die konventionelle Abformmethode (CO) und mit 21,9 [1,5] µm (PS) als den besten Wert für die digitale Abformmethode.
Schlussfolgerung: Unter Berücksichtigung der Einschränkungen dieser In-vitro-Studie können bestimmte digitale Intraoralscanner als Alternative zur konventionellen Abformung für Teilkieferbereiche gesehen werden. Ganzkieferabformungen sind nach wie vor eine Herausforderung für Intraoralscanner, aber einige Systeme liefern auch jetzt schon Genauigkeiten innerhalb der klinischen Anforderungen. Weitere In-vivo-Studien sind nötig, um diese Ergebnisse abzusichern.
Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro
Objective: Intraoral scanners (IOSs) are widely used for obtaining digital dental models directly from the patient. Additionally, improvements in IOSs are made from generation to generation. The aim of this study was to evaluate the accuracy of new and actual IOS devices for complete- and partial-arch dental impressions in an in vitro setup.
Materials and methods: A custom maxillary complete-arch cast with teeth made from feldspar ceramic material was used as the reference cast and digitized with a reference scanner (ATOS III Triple Scan MV60). One conventional impression technique using polyvinylsiloxane (PVS) material (President) served as the control (CO), and eight different IOS devices comprising different hardware and software configurations (TRn: Trios 3; TRi: Trios 3 insane; CS: Carestream Dental CS 3600; MD: Medit i500; iT: iTero Element 2; OC4: Cerec Omnicam 4.6.1; OC5: Cerec Omnicam 5.0.0; PS: Primescan) were used to take complete-arch impressions from the reference cast. The impressions were repeated 10 times (n = 10) for each group. Conventional impressions were poured with type IV gypsum and digitized with a laboratory scanner (inEos X5). All datasets were obtained in standard tessellation language (STL) file format and cut to either complete-arch, anterior segment, or posterior segment areas for respective analysis. Values for trueness and precision for the respective areas were evaluated using a three-dimensional (3D) superimposition method with special 3D difference analysis software (GOM Inspect) using (90–10)/2 percentile values. Statistical analysis was performed using either one-way analysis of variance (ANOVA) or Kruskal-Wallis test (α = 0.05). Results are given as median and interquartile range [IQR] values in µm.
Results: Statistically significant differences were found between test groups for complete- and partial-arch impression methods in vitro (p < 0.05). Values ranged from 16.3 [2.8] µm (CO) up to 89.8 [26.1] µm (OC4) for in vitro trueness, and from 10.6 [3.8] µm (CO) up to 58.6 [38.4] µm (iT) for in vitro precision for the complete-arch methods. The best values for trueness of partial-arch impressions were found for the posterior segment, with 9.7 [1.2] µm for the conventional impression method (CO), and 21.9 [1.5] µm (PS) for the digital impression method.
Conclusion: Within the limitations of this study, digital impressions obtained from specific IOSs are a valid alternative to conventional impressions for partial-arch segments. Complete-arch impressions are still challenging for IOS devices; however, certain devices were shown to be well within the required range for clinical quality. Further in vivo studies are needed to support these results.
Introduction
Digitalization of the alveolar arch using intraoral scanners (IOSs) represents a viable approach for obtaining digital dental models directly from the patient. Compared with conventional impression methods with irreversible materials, digital impression methods offer several advantages such as easy repeatability of the impression, direct visualization of the model, better time efficiency, and the possibility of chairside production for computer-aided design/computer-aided manufacturing (CAD/CAM) restorations.1-5 Intraoral scans can be further used within the digital dental workflow using data fusion options with other digital datasets, such as cone beam computed tomography (CBCT) scans and face scans.6,7 Three-dimensional (3D) difference analysis options based on intraoral scans have been demonstrated to offer great potential in terms of patient monitoring.8,9
The fact that the accuracy of digital impressions has been subject to several recent investigations demonstrates that there is still a need for scientific evidence in this field. For short-span areas such as single tooth areas and partial-arch areas such as quadrant and sextant areas, digital impressions have been demonstrated to perform within the same accuracy range as conventional impressions with high-precision materials.10-12 For long-span areas such as complete-arch, it has been demonstrated that there is a need for improvement of IOSs to reach the accuracy levels of conventional impressions.13-17 Shortcomings for digital impressions with IOSs have also been reported, both for edentulous and multi-implant clinical situations.18-20
Accuracy is defined by two independent factors: trueness and precision.21 Trueness is obtained by comparing the original geometry, ie, the reference master cast with the digitized model, while precision is obtained by an intragroup comparison of digitized models.21 High accuracy of dental models is needed to guarantee the sufficient fit of dental restorations and correct virtual articulation of the models.22,23
In literature, different approaches have been described for the evaluation of the accuracy of IOSs. Indirect approaches such as the evaluation of restoration fit have been described.24,25 Direct approaches through linear measurements on the dental arch geometries or 3D surface comparisons after best-fit alignment have also been described and are most commonly used for accuracy evaluations.26-28 It is important to emphasize that the correct method for accuracy measurements should be selected depending on the respective focus of interest, as there is not one approach that describes all the relevant factors. The interpretation of results for accuracy measurements always has to be based on very specific knowledge and assumptions in combination with a profound understanding of correct statistical data analysis.
There are well-known discrepancies for accuracy measurements between in vitro and in vivo accuracy studies using IOS devices.29,30 Factors such as the surface characteristics of scanned objects, oral environment factors, and patient movements might negatively influence the accuracy of IOSs in vivo.31,32 Determination of the in vivo trueness parameter is difficult because there is a lack of a reference master geometry. In vitro studies thus provide an insight into the possible accuracy of IOSs and might facilitate obtaining validity with a more in vivo-like test setup.33-35
The aim of the present study was to evaluate the accuracy of new and actual digital and conventional impression methods in vitro for complete- and partial-arch areas using a customized model simulating in vivo-like conditions in terms of tooth surfaces and optical characteristics. The null hypothesis of this study was that there are no statistically significant differences between different impression methods for complete- and partial-arch segments.
Fig 1 Customized complete-arch maxillary cast with teeth made from feldspar ceramic material (Cerec Blocs; Dentsply Sirona) that served as the reference cast.
Materials and methods
A custom maxillary complete-arch cast with unprepared teeth was used as a reference cast for the evaluation of in vitro accuracy. Teeth were made from feldspar ceramic material (Cerec Blocs; Dentsply Sirona) to approximate the optical properties of natural teeth (Fig 1).32,36,37 The reference cast was scanned with a high-resolution reference scanner (ATOS III Triple Scan MV60; GOM) to obtain a highly accurate digitized reference model.11
Eight different IOS setups comprising different hardware and software combinations were used in this study: Trios 3 Pod v. 1.18.2.6 (3Shape) using normal scan speed mode (TRn); Trios 3 Pod v. 1.18.2.6 (3Shape) using insane scan speed mode (TRi); Carestream Dental CS 3600 v. 3.1.0 (Carestream Dental [CS]) ; Medit i500 v. 1.2.1 (Medit [MD]); iTero Element 2 v. 1.7 (Align Technology [iT]); Cerec Omnicam v. 4.6.1 (Dentsply Sirona [OC4]); Cerec Omnicam v. 5.0.0 (Dentsply Sirona [OC5]); and Primescan v. 5.0.0 (Dentsply Sirona [PS]). Scans of the complete-arch cast were repeated 10 times per group (n = 10) using the manufacturers’ recommended scanning strategies. All scans were exported into binary standard tessellation language (STL) files for further processing.
Table 1 Test groups with respective impression techniques and software used to generate STL model files.
Conventional impressions of the reference cast were taken with stock metal trays (ASA Perma-Lock; ASA Dental) prepared with VPS universal adhesive (Coltène AG) and polyvinylsiloxane (PVS) material (President 360 heavy body and President light body; Coltène AG) using a one-step two-viscosity technique. This served as the control group (CO). The setting time for the impression material was 10 min, and the storage time prior to pouring the impressions with type IV gypsum (Fujirock EP; GC Corporation) was 8 h. Poured casts were stored for 24 h and subsequently digitized with an extraoral laboratory scanner (inEos X5; Dentsply Sirona). Conventional impressions were repeated 10 times (n = 10). Again, all scan data were exported into binary STL files. Table 1 summarizes the impression procedures of all the test groups. The online references for the respective scanning strategies used are given within the table, where these are available. All other scanning strategies can be found in the user manuals provided by the respective manufacturers.
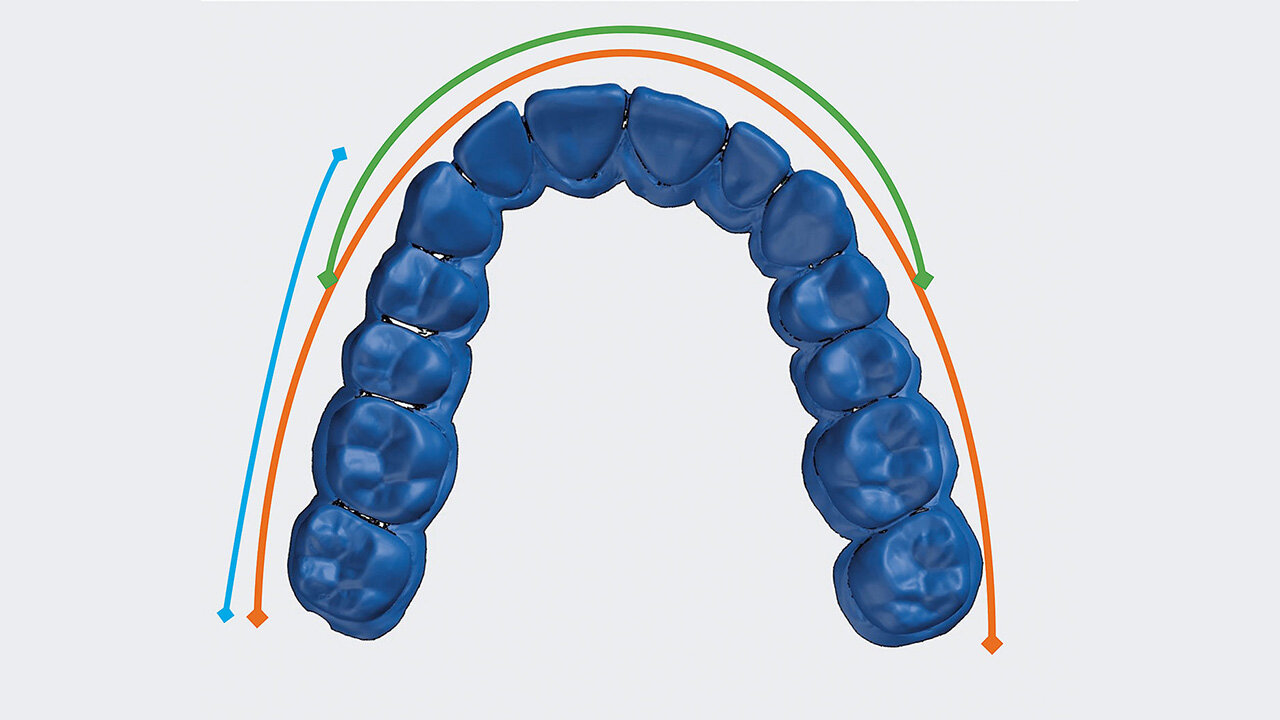
Fig 2 Digitized reference model (ATOS III Triple Scan MV60). The color-coded lines indicate the regions of interest for the in vitro accuracy evaluation: orange – complete-arch segment (tooth 17 to tooth 27), green – anterior segment (tooth 14 to tooth 24), blue – posterior segment (tooth 13 to tooth 17).
In the present study, three different regions of interest were used for the evaluation of accuracy of digital and conventional impression methods: complete-arch (tooth 17 to tooth 27); anterior segment (tooth 14 to tooth 24); and posterior segment (tooth 13 to tooth 17). The respective regions were selected from the digitized complete-arch dataset obtained for each group from the digitized complete-arch master model (Fig 2) (GOM Inspect 2018 rev. 114010; GOM).
The evaluation of accuracy started with a superimposition of the scans according to the method of best-fit alignment (GOM Inspect 2018 rev. 114010). After superimposition, 3D distances were calculated for each surface point and analyzed with 3D difference analysis software (GOM Inspect 2018 rev. 114010). Values for trueness (comparisons with reference scan; N = 10) and precision (intragroup comparisons; N = 45) for each group and for each respective area were calculated using (90–10)/2 percentile values. The results were evaluated using statistical software (SPSS 25; IBM), and descriptive statistic values were given as median with respective interquartile range [IQR] and mean ± standard deviation (SD) (all values in µm). Normal distribution and equality of variance were tested with the Shapiro-Wilk and Levene’s tests. Statistically significant differences were then calculated using either the Kruskal-Wallis test for non-normal distributed data or the one-way analysis of variance (ANOVA) with the post hoc Dunnett T3 test for normal distributed data (significance level α = 0.05).
Table 2 Results for trueness and precision values for digital and conventional impression methods using the (90-10)/2 percentile method.
Results
Results for the complete- and partial-arch impression methods in vitro including statistical analysis are shown in Figure 3, and in Table 2 as median with interquartile range (IQR) and mean ± standard deviation (SD) in µm. Values for trueness ranged from 16.3 [2.8] µm (CO) up to 89.8 [26.1] µm (OC4) for the complete-arch impressions, from 14.3 [2.3] µm (CO) to 68.4 [10.9] µm (MD) for the anterior segment, and from 9.7 [1.2] µm (CO) to 46.8 [4.9] µm (MD) for the posterior segment.
Fig 3 Boxplot diagrams showing the trueness and precision values for the digital and conventional impression methods using (90–10)/2 percentile values. The box represents the interquartile range [IQR]. The bar within the box represents the median value. Three different regions of interest were evaluated for each group: complete-arch, anterior segment, and posterior segment.
Precision values ranged from 10.6 [3.8] µm (CO) up to 58.6 [38.4] µm (iT) for the complete-arch impressions, from 7.8 [1.4] µm (CO) to 39.0 [18.3] µm (MD) for the anterior segment, and from 6.6 [1.4] µm (CO) up to 21.5 [8.6] µm (CS) for the posterior segment.
The conventional impression method (CO) showed significantly higher trueness (16.3 [2.8] µm) and precision (10.6 [3.8] µm) than all tested IOS devices for the complete-arch impressions. The IOS devices showed a great variability in terms of trueness and precision for the complete- and partial-arch segments. Within the IOS devices, group PS showed higher trueness (32.4 [9.8] µm) for the complete-arch impressions, with statistically significant differences to all the other IOS groups, except TRi. In the anterior segments, the lowest deviations concerning trueness for IOS devices were also found for group PS. Within the posterior region, PS, TRi, and TRn did not exhibit statistically significant differences to group CO for trueness.
Discussion
In this study, the accuracy of both new and actual digital impression methods and a conventional impression method in vitro for complete- and partial-arch segments was evaluated using a new customized model simulating in vivo-like conditions. There were eight different IOS setups comprising different hardware and software combinations, and one conventional impression method using PVS material served as a control. The evaluation of accuracy was performed using the superimposition method, with a best-fit alignment of digitized models and a difference analysis using 3D difference analysis software and (90–10)/2 percentile values. Results varied with regard to statistically significant differences among different test groups for accuracy of the complete- and partial-arch impression methods (p < 0.05). Based on the findings of this study, the null hypothesis that there are no statistically significant differences between different impression methods for complete- and partial-arch segments has to be rejected. The results of this study are discussed next according to various aspects.
In this study, clinically acceptable results for all IOS devices were found for partial-arch posterior segments with deviations below 50 µm for all test groups. These results support findings from previous studies and recently published review articles recommending digital intraoral impressions as a suitable alternative to conventional impression methods for this specific indication.30 In this study, the best results for complete- and partial-arch impression methods were found for group CO, both for the trueness and precision parameters. IOS devices showed the highest accuracy for posterior segments for all test groups compared with anterior segment and complete-arch impressions. Higher deviations of IOS devices for both the trueness and precision parameters were found for the anterior segment compared with the posterior segment, presumably caused by the specific morphological structure of anterior teeth, with only scant morphological information. Higher deviations within the anterior segment resulted in lower complete-arch accuracy for IOS devices.Group PS showed a higher trueness with significantly lower deviations compared with all the other IOS groups for the anterior segment. Within the posterior segment, PS, TRi, and TRn did not exhibit statistically significant differences to CO for trueness.
For some IOS devices, previous studies with similar evaluation methods report lower values in terms of complete-arch in vitro trueness.15,38 This may be related to the use of a different reference cast (stainless steel) with non-translucent tooth surfaces.15,38 The higher deviations observed in the present study might be caused by the translucent surface of the cast teeth made from feldspar ceramic material (Cerec Blocs). Feldspar ceramic shows natural tooth-like scanning behavior due to its natural tooth-like translucency.32,36,37 It seems important to emphasize this fact because it might influence the comparability of different in vitro studies that use different reference cast materials. Interestingly, the results of the present study for in vitro precision of complete-arch impressions were within the same range as previously published results for in vivo complete-arch precision for some IOS devices.39
In this study, a 3D surface comparison approach using (90–10)/2 percentile values was used, following a well-established protocol.15,40 It is difficult to compare the results of this study directly with the results of other studies that used different statistical interpretations and distance measurements. There are different evaluation methods for the accuracy of dental impressions depending on different kinds of measures for trueness and precision. For the linear evaluation approach, an exact determination of specific reference points is a major requirement. This approach is thus preferred for accuracy evaluations of defined geometries with defined sharp edges or knots such as implant scan bodies or other geometrical objects. In the case of freeform surfaces such as teeth and anatomical structures, this procedure is generally not recommended. Therefore, 3D surface comparison approaches are used for real comparisons of freeform surfaces such as natural tooth surface morphology, which comprises thousands of linear surface distance point measurements. The superimposition of digitized models with best-fit algorithms is the standard procedure for 3D surface comparisons. However, there are also multiple different ways to summarize the 3D-difference values, which result from the pointwise distance calculations of the superimposed surfaces. Examples from the most recent literature are root mean square (RMS) error, mean value, and positive and negative (absolute) mean deviation. The amount of incorporated measurement data and therefore the region of interest is different for all these evaluations, which makes it difficult to compare the results of different studies.10-12
The influence of scanning strategies and scanning software on the accuracy of digital impressions has been demonstrated in the literature.14,41 Scanning strategies for IOS devices are system specific, as IOSs are based on different technologies. A system-specific scanning strategy with actual scanning software for every IOS device was used in this study to obtain optimal results. The influence of the scanning software is apparent when comparing the results of groups OC4/OC5, where the same hardware components but different scanning software modes/versions were used. Previous studies show increasing deviations for trueness and precision with an increasing area of scanned surface for IOS devices, whereas this statement cannot be made for conventional impression methods.10-12,39,42 The results of this study accord well with this statement. Short-span areas such as the anterior and posterior segments showed the lowest deviation values for IOS devices, whereas only small differences were found between partial- and complete-arch accuracy for the conventional impression methods.
Conclusion
Accuracy for complete-arch impressions is still challenging for specific IOS devices. Certain actual IOS devices, however, are well within the required accuracy necessary for full-arch scans. In case of partial-arch impressions, IOS devices represent a suitable alternative to conventional impression methods even with highly accurate impression materials. The results of the present study show that new hardware and/or software developments can provide major improvements in terms of impression accuracy for IOS devices. Further in vivo studies are needed to validate the accuracy of IOS devices under different clinical conditions.
Disclaimer
The authors declare that there are no conflicts of interest.
PD Dr. med. dent. Andreas Ender, Dr. med. dent. Moritz Zimmermann und Prof. Dr. med. dent. Dr. rer. hum. biol. Albert Mehl, Zürich
1. Reich S, Vollborn T, Mehl A, Zimmermann M. Intraoral optical impression systems – an overview. Int J Comput Dent 2013;16:143–162.
2. Patzelt SB, Lamprinos C, Stampf S, Att W. The time efficiency of intraoral scanners: an in vitro comparative study. J Am Dent Assoc 2014;145:542–551.
3. Yuzbasioglu E, Kurt H, Turunc R, Bilir H. Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014;14:10.
4. Zimmermann M, Mehl A, Mörmann WH, Reich S. Intraoral scanning systems – a current overview. Int J Comput Dent 2015;18:101–129.
5. Sfondrini MF, Gandini P, Malfatto M, Di Corato F, Trovati F, Scribante A. Computerized casts for orthodontic purpose using powder-free intraoral scanners: accuracy, execution time, and patient feedback. Biomed Res Int 2018;2018:4103232. doi: 10.1155/2018/4103232.
6. Joda T, Gallucci GO. The virtual patient in dental medicine. Clin Oral Implants Res 2015;26:725–726.
7. Mangano C, Luongo F, Migliario M, Mortellaro C, Mangano FG. Combining intraoral scans, cone beam computed tomography and face scans: the virtual patient. J Craniofac Surg 2018;29:2241–2246.
8. Mehl A, Koch R, Zaruba M, Ender A. 3D monitoring and quality control using intraoral optical camera systems. Int J Comput Dent 2013;16:23–36.
9. Zaruba M, Ender A, Mehl A. New applications for three-dimensional follow-up and quality control using optical impression systems and OraCheck. Int J Comput Dent 2014;17:53–64.
10. Vecsei B, Joós-Kovács G, Borbély J, Hermann P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems – an in vitro study. J Prosthodont Res 2017;61:177–184.
11. Renne W, Ludlow M, Fryml J, et al. Evaluation of the accuracy of 7 digital scanners: an in vitro analysis based on 3-dimensional comparisons. J Prosthet Dent 2017;118:36–42.
12. Serag M, Nassar TA, Avondoglio D, Weiner S. A comparative study of the accuracy of dies made from digital intraoral scanning vs. elastic impressions: an in vitro study. J Prosthodont 2018;27:88–93.
13. Ender A, Mehl A. Full arch scans: conventional versus digital impressions – an in-vitro study. Int J Comput Dent 2011;14:11–21.
14. Ender A, Mehl A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int J Comput Dent 2013;16:11–21.
15. Ender A, Mehl A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int 2015;46:9–17.
16. Su TS, Sun J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: An in-vitro study. J Prosthodont Res 2015;59:236–242.
17. Jeong ID, Lee JJ, Jeon JH, Kim JH, Kim HY, Kim WC. Accuracy of complete-arch model using an intraoral video scanner: an in vitro study. J Prosthet Dent 2016;115:755–759.
18. Patzelt SB, Vonau S, Stampf S, Att W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J Am Dent Assoc 2013;144:914–920.
19. Vandeweghe S, Vervack V, Dierens M, De Bruyn H. Accuracy of digital impressions of multiple dental implants: an in vitro study. Clin Oral Implants Res 2017;28:648–653.
20. Fang JH, An X, Jeong SM, Choi BH. Digital intraoral scanning technique for edentulous jaws. J Prosthet Dent 2018;119:733–735.
21. Ender A, Mehl A. Accuracy in dental medicine, a new way to measure trueness and precision. J Vis Exp 2014;86. doi: 10.3791/51374.
22. Patzelt SB, Emmanouilidi A, Stampf S, Strub JR, Att W. Accuracy of full-arch scans using intraoral scanners. Clin Oral Investig 2014;18:1687–1694.
23. Zimmermann M, Ender A, Attin T, Mehl A. Accuracy of buccal scan procedures for the registration of habitual intercuspation. Oper Dent 2018;43:573–580.
24. Memari Y, Mohajerfar M, Armin A, Kamalian F, Rezayani V, Beyabanaki E. Marginal adaptation of CAD/CAM all-ceramic crowns made by different impression methods: a literature review [epub ahead of print 20 April 2018]. J Prosthodont 2018. doi: 10.1111/jopr.
25. Bosniac P, Rehmann P, Wöstmann B. Comparison of an indirect impression scanning system and two direct intraoral scanning systems in vivo [epub ahead of print 9 Oct 2018]. Clin Oral Investig 2018. doi 10.1007/s00784-018-2679-4.
26. Guth JF, Edelhoff D, Schweiger J, Keul C. A new method for the evaluation of the accuracy of full-arch digital impressions in vitro. Clin Oral Investig 2016;20:1487–1494.
27. Tomita Y, Uechi J, Konno M, Sasamoto S, Iijima M, Mizoguchi I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent Mater J 2018;37:628–633.
28. Ender A, Mehl A. Accuracy of complete-arch dental impressions: a new method of measuring trueness and precision. J Prosthet Dent 2013;109:121–128.
29. Goracci C, Franchi L, Vichi A, Ferrari M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: a systematic review of the clinical evidence. Eur J Orthod 2016;38:422–428.
30. Khraishi H, Duane B. Evidence for use of intraoral scanners under clinical conditions for obtaining full-arch digital impressions is insufficient. Evid Based Dent 2017;18:24–25.
31. Nedelcu RG, Persson AS. Scanning accuracy and precision in 4 intraoral scanners: an in vitro comparison based on 3-dimensional analysis. J Prosthet Dent 2014;112:1461–1471.
32. Kurz M, Attin T, Mehl A. Influence of material surface on the scanning error of a powder-free 3D measuring system. Clin Oral Investig 2015;19:2035–2043.
33. Kuhr F, Schmidt A, Rehmann P, Wöstmann B. A new method for assessing the accuracy of full arch impressions in patients. J Dent 2016;55:68–74.
34. Atieh MA, Ritter AV, Ko CC, Duqum I. Accuracy evaluation of intraoral optical impressions: a clinical study using a reference appliance. J Prosthet Dent 2017;118:400–405.
35. Park HN, Lim YJ, Yi WJ, Han JS, Lee SP. A comparison of the accuracy of intraoral scanners using an intraoral environment simulator. J Adv Prosthodont 2018;10:58–64.
36. Yu B, Ahn JS, Lee YK. Measurement of translucency of tooth enamel and dentin. Acta Odontol Scand 2009;67:57–64.
37. Della Bona A, Nogueira AD, Pecho OE. Optical properties of CAD-CAM ceramic systems. J Dent 2014;42:1202–1209.
38. Muller P, Ender A, Joda T, Katsoulis J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int 2016;47:343–349.
39. Ender A, Attin T, Mehl A. In vivo precision of conventional and digital methods of obtaining complete-arch dental impressions. J Prosthet Dent 2016;115:313–320.
40. Zimmermann M, Koller C, Rumetsch M, Ender A, Mehl A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J Orofac Orthop 2017;78:466–471.
41. Haddadi Y, Bahrami G, Isidor F. Effect of software version on the accuracy of an intraoral scanning device. Int J Prosthodont 2018;31:375–376.
42. Ender A, Zimmermann M, Attin T, Mehl A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin Oral Investig 2016;20:1495–1504.
Adblocker aktiv! Bitte nehmen Sie sich einen Moment ...
Unser System meldet, dass Sie eine aktive AdBlocker-Software verwenden, die verhindert dass alle Seiteninhalte geladen werden können.
Fair geht vor: Unsere Partner aus der Industrie tragen durch ihre Anzeigen einen maßgeblichen Teil zum Betreiben dieser Newsseite bei. Diese finden Sie in überschaubarer Anzahl auf der Startseite sowie den einzelnen Artikelseiten.
Bitte setzen Sie www.quintessence-publishing.com auf Ihre „AdBlocker Whitelist“ oder deaktivieren Ihre AdBlocker Software. Danke.
Was bringt der Hessische Zahnärztetag/Kongress Orale Medizin 24? – im Gespräch mit den Wissenschaftlichen Leitern Prof. Jan-Frederik Güth und Muzafar Bajwa M.Sc.